Conditions that may present with CHD
1.Ventricular Septal Defect (VSD)

Examination/Investigation findings
- Examination:
- They are usually asymptomatic and undetectable unless large.
- Large lesions are defined as being the same size or larger than the aortic valve and larger lesions are often associated with pulmonary hypertension and present with CCF after one week
- May have pansystolic murmur at lower left sternal edge usually the louder the murmur the smaller the hole
- Investigations:
- ECG: Biventricular hypertrophy by 2 months
- CXR: shows increased pulmonary vascular markings and cardiomegaly
Management
- Trial of medical management
- Loop diuretics such as Furosemide, Digoxin, ACE-inhibitors, Beta-blockers and Spironolactone are used.
- Supplemental oxygen and hyperventilation should be avoided as they will cause pulmonary vascular resistance to fall which causes increased shunting.
- Muscular VSDs often close spontaneously whereas perimembranous VSDs do not.
- These are closed either surgically or via percutaneous closure by an interventional cardiologist.
- Surgical correction is deferred to 3-5 months of age, as this has been shown to improve outcome.
- Atrial Septal Defect (ASD)


Examination/investigation findings
- Examination: Soft systolic murmur at upper sternal edge
- ECG: Partial RBBB, RV hypertrophy
- CXR: Cardiomegaly, increased pulmonary vascular markings
Management
- Medical management is used to treat symptoms of CCF.
- Surgical closure usually occurs at 3-5 years of age
- 90% undergo device closure in catheter lab , 10% undergo surgical closure if defects are large
Learning bite
ASDs and VSDs are managed medically to allow surgical closure to be deferred as this improves outcomes.
- Patent Ductus Arteriosus (PDA)
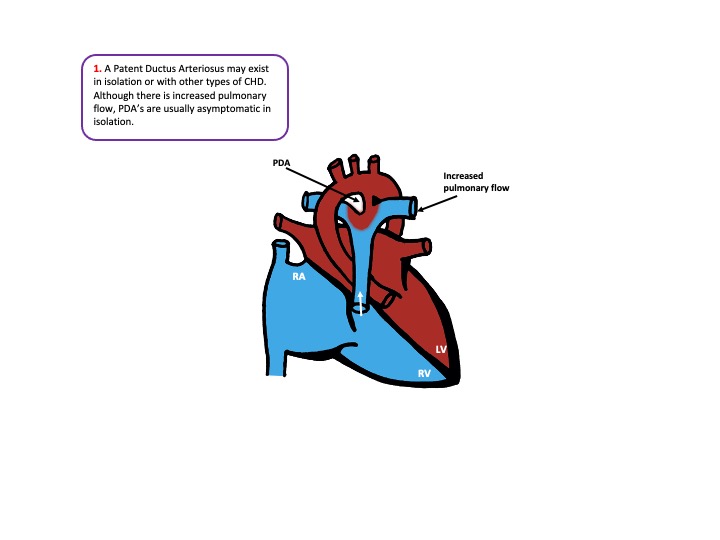

Examination/investigation
- Examination: Continuous systolic murmur in the left infraclavicular area known as a machinery murmur
- Investigations
- ECG: Usually normal
- CXR: Increased pulmonary vascular markings if large
Management
- 2/3rds PDAs will close with a course of indomethacin or Ibuprofen as these are prostaglandin inhibitors
- If large enough to cause CCF medical management is used and surgical ligation is carried out at 1-3 months
- If there is no CCF closure in catheter lab with a coil or device is carried out at 1 year
- There is a slightly increased risk of bacterial endocarditis if left patent
Learning bite
PDAs rarely cause symptoms in children – they are often picked up incidentally from the murmur.