Primary Triage
The purpose of primary triage at a major incident is not to provide medical care but rather to identify patients in need of life-saving intervention by other healthcare providers. There are generally two exceptions to the ‘triage not treatment’ rule (5):
- Provision of basic airway manoeuvres/adjuncts if a patient is not breathing
- Application of a Combat Application Tourniquet (CAT) for catastrophic haemorrhage
The MPTT-24
Primary triage, commonly referred to as the ‘triage sieve’, is generally performed using a validated algorithm such as the Modified Physiology Triage Tool (MPTT-24) (6). This has advantages in that it does not need to be performed by a person with a high level of medical training and could be effectively delegated to any competent person at the scene of the incident. It may in fact be advantageous for team members with less medical knowledge to undertake primary triage, as they are more likely to comply with the protocol and less likely to be distracted by other tasks or interventions. The triage sieve aims to be objective and readily reproducible. However, in common with all tools of its type, it does not take account of a patients likely course and may miss patients who are wholly salvageable – for example a patient with airway burns may initially be walking and triaged a P3, but a short time later develop airway occlusion, and may die if they are not quickly identified and re-triaged for more urgent care.
The MPTT-24 triage tool can be seen below to be a simple flow chart. It considers the presence or absence of catastrophic haemorrhage, the patients ambulatory status, their responsiveness, and simple observations of their pulse and respiratory rate. Following the algorithm through, it is evident that with a maximum of six questions, the patient can be easily allocated to their triage category. They are immediately marked and (with the exceptions noted above), the person performing triage moves on to assess the next patient without executing any medical intervention.
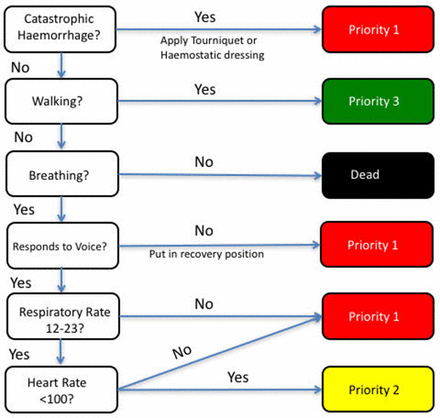
Fig 3: MPTT-24 Modified Physiological Triage Tool (6)