
Author: Sarah Stobbs / Editor: Janet Skinner, Ravi Tota Maharaj / Reviewer: Joe Schrieber, Caitriona Considine / Codes: CC10, CC5 / Published: 09/03/2020 / Reviewed: 11/05/2026
Context
Alcohol abuse is undoubtedly a huge social problem in the UK. It is responsible for many unnecessary attendances to the emergency department (ED) and is an enormous burden on the NHS, which must treat the complications of alcohol abuse. UK Chief Medical Officers advise that, to keep health risks low, men and women should not regularly drink more than 14 units per week, and if drinking up to this level, it is best spread evenly over 3 or more days. [1]
In 2023, 10,473 alcohol-specific deaths were registered in the UK (15.9 deaths per 100,000 people) a 4.2% increase from 2022. Alcoholic liver disease accounted for 75.6% of all alcohol-specific deaths. Male deaths remain twice as high as female deaths. [2]
Scotland has the highest alcohol-specific death rate among the UK nations. Rates are 4.5 times higher in deprived areas.
Alcohol-related liver disease accounts for over 60% of alcohol-related deaths and is now the leading cause of liver transplantation in the UK. [2]
Definition
Alcohol-Related Liver Disease (ArLD) is a clinical and histological spectrum of diseases which includes fatty liver (FL) at one extreme and alcohol-related cirrhosis at the other. [3,4]
Fatty liver is generally benign and asymptomatic and occurs in patients who abuse alcohol for a period of days to weeks. It is entirely reversible with abstinence from alcohol. However, with susceptibility and continued alcohol abuse, more advanced disease can develop with alcohol-related hepatitis, an inflammation of the liver, which can lead to, or exist with alcohol-related cirrhosis, in which the liver can become fibrosed.

Fig 1: Spectrum of damage in alcoholic liver disease.
Learning Bite
ArLD can be thought of as a spectrum from reversible fatty liver to alcoholic hepatitis to alcoholic cirrhosis.
Basic Science and Pathophysiology
Pathogenesis of Alcohol-Related Liver Disease (ArLD)
Alcohol causes damage to the liver by various mechanisms, which can be exacerbated by other factors.
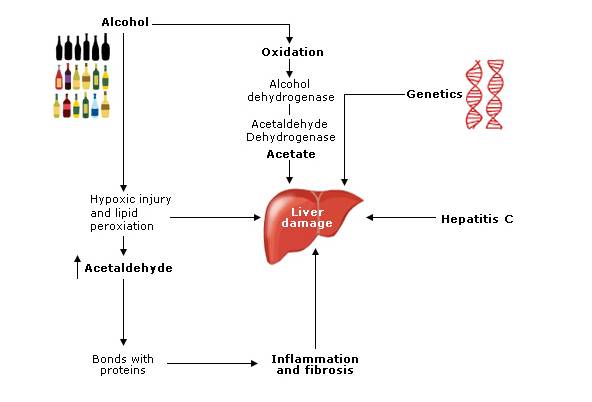
Acetaldehyde direct hepatocyte damage
Acetaldehyde concentration is increased in the liver with sustained alcohol intake resulting in hepatocytes becoming susceptible to hypoxia and hypoxic injury. Oxygen free radicals cause injury to hepatocytes by lipid peroxidation. [3]
Genetics
Genetic factors have been implicated by studies which have found a relationship between ArLD and polymorphisms of alcohol metabolising enzyme systems (ALDH2, Cytochrome p450) and cytokines (TNF, IL1, IL10). [5]
Acetate altered carbohydrate metabolism
The metabolism of ethanol (alcohol) occurs in the mitochondria where it is oxidised to alcohol dehydrogenase. This is then oxidised to acetate by acetaldehyde dehydrogenase. These reactions alter the redox state of the cell and can have detrimental effects on lipid and carbohydrate delivery, metabolism and export from the liver causing triglyceride accumulation (fatty liver). [3,6]
Hepatitis C
Hepatitis C infection and alcohol have an additive effect together. This is thought to occur as alcohol may alter the immune systems efforts at clearing the virus, or increased iron deposition in liver secondary to high levels of alcohol which may alter the pathophysiology of the virus. [3]
Hepatitis C and ArLD also increases the chance of developing hepatocellular carcinoma significantly. [6]
Learning Bite
Development of ArLD is mutifactorial and includes sex, hepatitis infections and genetics.
Inflammatory response
Acetaldehyde forms covalent bonds with proteins which are antigenic. Long-term exposure to alcohol causes the body to amass circulating antibodies to these proteins resulting in harmful humeral and cellular responses.
In alcohol-related liver injury the expression of pro-inflammatory cytokines is up-regulated resulting in fibrosis. [3] Collagen is deposited in the space of disse, which progresses to fibrosis and cell linkage formation resulting in cirrhosis. Lesions occur in the hepatic veins causing thickened veins and perisinusoidal fibrosis, [6] which can lead to cirrhosis.
Clinical Features
Such liver damage can be potentially life-threatening:
- Alcohol-related hepatitis can result from prolonged alcohol abuse and presents with non-specific systemic symptoms; and can also cause features of portal hypertension
- Alcohol-related cirrhosis results in severe liver injury and shrinkage with increased portal hypertension and associated complications as well as decline of liver synthetic function. [7]
It is important to remember that alcohol can cause significant damage to the liver and health in general without producing any physical signs or symptoms. A vast majority of patients are diagnosed on routine blood tests.
Symptoms
Early symptoms may be non-specific and thus can require a certain clinical acumen to diagnose. More advanced disease may present with typical signs of liver disease. Sequelae of alcohol abuse may also be the presenting complaint, such as injuries. [3]
Clinical history
An open mind is required for all patients, especially within the ED, and alcohol intake should be part of every clinical history, although patients may be unaware that their intake is high or may deny the problem. Collateral history is often important in these situations.
The Spectrum of Alcoholic Liver Disease
Symptomatic
The majority of cases of early liver damage can be diagnosed incidentally on routine blood tests in the ED or primary care. Many patients with fatty liver will be asymptomatic, hepatomegaly on examination may be the only finding.
Early symptoms of Alcohol-Related Liver Disease
The majority of early symptoms of sustained alcohol abuse are generally non-specific symptoms, such as abdominal discomfort, vomiting or anxiety.
Injuries associated with intoxication
Often the first attendance to the ED of patient with potential ArLD is due to a consequence of alcohol, such as falls, rib fractures, head injury or domestic violence.
Cirrhosis
This is the end point of liver damage and is when the liver tissue is replaced by scar tissue due to the sustained damage caused by alcohol.
The synthetic function of the liver is compromised leading to bleeding and metabolic complications together with complications of portal hypertension mentioned previously.
Portal hypertension
Clinical findings in portal hypertension are caused by blood being forced down different channels as the portal system pressure rises due to liver damage. Signs include ascites, varices (rectal and oesophageal), dilated abdominal veins, caput medusa with the risk of developing encephalopathy.
Alcohol-related hepatitis
These patients will often look more unwell with pyrexia and anorexia. Their liver function tests will be deranged and they may have clinical signs of chronic liver damage.
Screening Tools
Screening tools for use in the ED include:
AUDIT-C (Alcohol Use Disorders Identification Test Consumption) This is the recommended first-line screening tool in UK emergency care. It comprises three questions about frequency of drinking, quantity consumed on a typical day, and frequency of heavy drinking ( 6 units per occasion).
A score of 5 in men or 4 in women indicates hazardous drinking requiring intervention.
FAST (Fast Alcohol Screening Test) is a four-item screening tool derived from AUDIT, useful for rapid ED assessment. A score of 3 indicates hazardous drinking. [8]

The Paddington Alcohol Test (PAT) Specifically designed for ED settings to identify hazardous drinkers presenting with alcohol-related injuries or conditions. [9]
CAGE questionnaire While historically used, this is less sensitive than AUDIT-C for detecting hazardous drinking and is better suited to identifying alcohol dependence rather than risky consumption patterns.
The CAGE questionnaire is a useful screening tool.
| C Have you ever felt the need to cut down your drinking? |
| A Have you ever felt annoyed by criticism of your drinking? |
| G Have you ever felt guilty about your drinking? |
| E Have you ever taken a drink (eye opener) first thing in the morning? |
Yes to two or more of the above suggests alcohol excess.
Learning Bites
- Screening questionnaire tools should be used to identify problem drinking in the Emergency Department.
- AUDIT-C is the recommended first-line tool, with FAST and PAT as alternatives depending on clinical context.
Management in the ED
The essential component of management in the ED includes recognising problem drinkers by including alcohol history in all assessments, especially in alcohol related injuries and suspected ArLD.
A brief 10 minute opportunistic advice conversation with those found to have hazardous drinking (5 units per day for men or 3 units per day for women) has been found to be beneficial in raising awareness and reducing alcohol intake before it becomes harmful. [10]
Learning Bite
Brief interventions in the ED are effective in reducing alcohol intake.
Symptoms and Signs
Fatty Liver
Patients with FL are usually well. Hepatomegaly on examination may be the only sign of liver disease found. [3]
Alcohol-related hepatitis
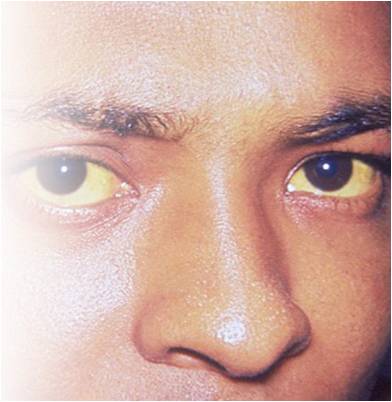
Fig. 3 Image via Wikimedia Commons
Patients suffering from alcohol-related hepatitis often look unwell with pyrexia. They can be jaundiced and show cutaneous signs of chronic liver damage (Fig 1). Tender hepatomegaly is found on palpation. Ascites and encephalopathy can develop but varices are rare, although bleeding may arise from gastric erosions exacerbated by coagulopathy. [3]
Alcohol-related cirrhosis
Features of alcohol-related cirrhosis include spider naevi, enlarged parotid glands, gynaecomastia, ascites, splenomegaly, palmar erythema, peripheral neuropathy and testicular atrophy. [3,6] Portal blood flow together with hepatic vascular resistance are both increased secondary to alcohol consumption, which increases portal pressure and collateral blood flow, thus increasing the risk of variceal bleeding in patients with alcoholic cirrhosis and increased portal hypertension. [3]
Learning Bite
Clinical signs of liver disease may be subtle even with significant pathology.
Risk Stratification
One unit of alcohol is equivalent to 8 g of ethanol (half pint of beer at 3.5% or 25 ml of spirits). Hazardous drinking is defined as regular daily consumption of over 5 units of alcohol for men (>40 g) and over 3 units for women (>24 g). Harmful drinking causes damage to physical or mental health.
Alcohol dependence is behaviour centred on the need to drink alcohol. [9] Evidence suggests drinking 60-80 g per day of alcohol for men and >20 g per day for women increases the risk of ArLD. Although studies have shown that a low number of patients (13.5%) with alcohol intake >120 g per day developed ArLD.
Risk factors
Clearly there are risk factors which increase the likelihood of ArLD happening, such as:
- Age
- Gender
- Genetics
Alcohol-related cirrhosis occurs in only 8-20% of alcoholic patients and Alcohol-related hepatitis in 6-30%.
The prognosis (long-term) improves with abstinence; the five year survival rate for those with compensated cirrhosis who continue to abuse alcohol is less than 70% with survival of >90% if they stop drinking. Decompensated liver disease survival drops to 30% in five years for those still drinking alcohol. [6]
Learning Bite
Prognosis in all stages of ALD improves with abstinence from alcohol.
In suspected severe alcohol-related hepatitis, clinicians should be aware that specialist teams use prognostic tools such as Maddrey Discriminant Function, Glasgow Alcoholic Hepatitis Score, and increasingly MELD, to support decisions about corticosteroids and escalation. [10]
Biomechanical Tests
Serum biochemical tests are useful for the diagnosis of alcohol-related liver disease:
Aspartate aminotransferase/alanine aminotransferase
Aspartate aminotransferase (AST)/alanine aminotransferase (ALT) ratio >2 differentiates between ArLD and other liver pathology. Impaired ALT rise results from a hepatic deficiency of pyridoxal-6-phosphate required for ALT enzyme activity in the liver. [6]
Gamma-glutamyltransferase
Gamma-glutamyltransferase (GGT) is often found to be raised. These markers assess alcohol abuse indirectly by testing liver damage and therefore have a low sensitivity and specificity of less than 70%.
Mean corpuscular volume
Mean corpuscular volume (MCV) is also found to be raised in most cases due to toxic effects of alcohol on bone marrow. This marker also has low sensitivity in the region of 50%.
Prolongation of the prothrombin time
Prolongation of the prothrombin time (PT) and low albumin levels suggest poor synthetic liver function. [6]
Thrombocytopenia may be an early indirect marker of advanced fibrosis or portal hypertension and can precede more obvious synthetic dysfunction.
The emerging tests below are sometimes used in conjunction with the tests above:
Carbohydrate-deficient transferrin test
Carbohydrate-deficient transferrin test shows the desialylation of transferrin which occurs in the presence of high alcohol intake independent of liver damage. This is thought to be specific for ArLD, although it has relatively low sensitivity.
Mitochondrial aminotransferase
Mitochondrial aminotransferase (AFT) is released from hepatocytes with sustained alcohol abuse.
Diagnosis
- Ratio of AST/ALT 1.5:2
- Low albumin
- High PT
- High MCV
- Low platelets
Other Tests
Imaging and Non-invasive Assessment
Transient Elastography (FibroScan) is now widely used in UK pathways as a routine non-invasive tool to assess liver stiffness (fibrosis) and steatosis in alcohol-related liver disease. It provides immediate results at the bedside or outpatient clinic and helps stratify patients into mild fibrosis, significant fibrosis, or cirrhosis without invasive procedures. [11]
Ultrasound remains helpful to investigate liver damage. Fatty liver and alcoholic hepatitis are demonstrated by changes in liver parenchymal reflectivity. A cirrhotic liver appears irregular and shrunken. Doppler studies may show slow or reversed portal vein flow, splenomegaly and intra-abdominal varices indicating portal hypertension.
Liver biopsy is reserved for cases where diagnostic uncertainty remains after non-invasive testing, or where important clinical information cannot be obtained by safer non-invasive means (such as differentiating between alcohol-related hepatitis and other causes of acute liver injury). In patients with coagulopathy, the transjugular venous route is preferred. [11]
Thiamine Deficiency
Current UK practice suggests that patients at risk of Thiamine deficiency dependent drinkers, malnourished patients and those with vomiting or suspected Wernickes, should receive parenteral thiamine, usually IV Pabrinex, rather than relying on oral thiamine alone. Oral thiamine is more appropriate for ongoing maintenance.
The key teaching point that thiamine should be given before glucose where possible should be retained. [12]
Investigation
Patients should be investigated appropriately in the ED using blood tests and imaging as available. ED doctors should act on abnormal blood results and seek help from specialists. Appropriate patients should then be referred to GI for ongoing management. Patients displaying evidence of advanced or acute disease should be admitted under the gastrointestinal (GI) physicians for specific management.
Most patients who are withdrawing from alcohol can be managed at home with no drugs or small doses of benzodiazepines for withdrawal. Patients at high risk of complicated withdrawal may benefit from a short inpatient stay to monitor them and adjust their drug doses as appropriate.
Observational studies have shown a strong correlation between involvement in Alcoholics Anonymous and long-term abstinence. [7] If patients present to the ED requesting detoxification, they should be advised to make an appointment with their GP and be given contact information for community support organisations.
All patients with suspected alcohol-related hepatitis, decompensated cirrhosis, or possible liver failure should have early discussion with gastroenterology/hepatology and infection screening in decompensated disease.
Management of Alcoholic Liver Disease
The essential part of successful management of ArLD is abstinence from alcohol. Fatty liver can be entirely reversible and other later presentations can be stabilised and improved with cessation of alcohol.
Corticosteroids are not a routine ED treatment for all patients. In selected severe alcohol-related hepatitis, steroids may provide a modest improvement in 28-day survival, but there is no sustained benefit at 90 days or 1 year, and treatment carries infection risk. Steroid use should therefore be specialist-led decision following infection screening and formal severity assessment. [11]
Nutritional support should also be given greater prominence, as malnutrition is common and clinically important in severe disease.
Studies have shown patients who had at least 2500 kcal per day had improvements in liver function and six month survival than those who had less. Enteral feeding maximises digestion and may improve long-term survival in ArLD patients. Interestingly, although obesity can be an independent risk factor for ArLD progression, weight loss has not been shown to be of benefit in alcoholic fatty liver disease and may actually worsen liver injury. [6]
Learning Bite
At all stages of ALD, abstinence is key to management.
Ongoing Management
Provide written information to the patient and family upon discharge. Ensure follow up with alcohol care teams and hepatology.
Complications of portal hypertension
As with other types of liver disease, complications of portal hypertension should be considered and managed appropriately, such as:
- Encephalopathy
- Oesophageal varices
- Ascites and liver synthetic function derangement
- Hypoglycaemia
- Coagulopathy
Caution should be taken when diagnosing encephalopathy in this patient group as the differentials include subdural haematoma, Wernickes encephalopathy and delirium tremens. [3]
Liver transplantation
Liver transplantation is the only curative treatment for advanced ArLD, however current or recent substance abuse is a contraindication for transplant. Selection requires a multi-disciplinary team approach including a hepatologist, surgeon, addiction specialist, psychiatrist and social worker. Patients must be motivated and compliant with immunosuppressive treatment. [7]
Transplant assessment principles updated to acknowledge that the old absolute six-month abstinence rule is no longer universally applied in the same rigid way, and that selected severe non-responders may be considered for early transplant assessment in specialist settings.
Learning Bite
Liver transplant is the only hope for cure in advanced ALD.
- Failing to question patients about alcohol intake when they present to the ED
- Not acting on abnormal blood results on asymptomatic patients
- Failing to refer patients to alcohol support services or a GI specialist when appropriate
- Failing to give thiamine to a patient suspected of alcoholism
- Under-treating thiamine deficiency risk by prescribing oral thiamine alone in vomiting, malnourished or dependent drinkers.
- Not recognising more serious aspects such as development of Wernickes encephalopathy or pathology secondary to alcohol related injuries, such as a subdural haematoma.
- Severe alcohol-related hepatitis is a life-threatening condition which requires urgent specialist discussion and consideration of disease-specific therapy.
- Department of Health. UK Chief Medical Officers low risk drinking guidelines. London: Department of Health; 2016. [cited 11 April 2026].
- Office for National Statistics (ONS). Alcohol-specific deaths in the UK: registered in 2023 [Internet]. Newport: ONS; 2025.
- Walsh K, Alexander G. Alcoholic liver disease. Postgrad Med J. 2000 May;76(895):280-6.
- Parker R, Aithal GP, Becker U, et al. Quality standards for the management of alcohol-related liver disease: consensus recommendations from the British Association for the Study of the Liver and British Society of Gastroenterology ALD Special Interest Group. BMJ Open Gastroenterol [Internet]. 2023;10(1):e001221
- Reuben A. Alcohol and the liver. Curr Opin Gastroenterol. 2006 May;22(3):263-71.
- Mndez-Snchez N, et al. Alcoholic liver disease. An update. Ann Hepatol. 2005 Jan-Mar;4(1):32-42.
- Menon KV, Gores GJ, Shah VH. Pathogenesis, diagnosis, and treatment of alcoholic liver disease. Mayo Clin Proc. 2001 Oct;76(10):1021-9.
- Parker A J R, et al. Diagnosis and management of alcohol use disorders. BMJ 2008; 336 :496
- Smith SG, et al. Detection of alcohol misusing patients in accident and emergency departments: the Paddington alcohol test (PAT). J Accid Emerg Med. 1996 Sep;13(5):308-12.
- National Institute for Health and Care Excellence (NICE). Alcohol-use disorders: diagnosis, assessment and management of harmful drinking (high-risk drinking) and alcohol dependence. [CG115] NICE. Last updated: 21 October 2014.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of alcohol-related liver disease. J Hepatol. 2018 Jul;69(1):154-181.
- Specialist Pharmacy Service (SPS). Using and prescribing thiamine in alcohol dependence. SPS / NHS. 2025.
- National Institute for Health and Care Excellence (NICE). Cirrhosis in over 16s: assessment and management. [NG50]. NICE. Last updated: 08 September 2023.
- Thursz MR, Richardson P, Allison M, Austin A, Bowers M, Day CP, Downs N, Gleeson D, MacGilchrist A, Grant A, Hood S, Masson S, McCune A, Mellor J, OGrady J, Patch D, Ratcliffe I, Roderick P, Stanton L, Vergis N, Wright M, Ryder S, Forrest EH; STOPAH Trial. Prednisolone or pentoxifylline for alcoholic hepatitis. N Engl J Med. 2015 Apr 23;372(17):1619-28.