
Author: Liz Herrieven / Editor: Nikki Abela / Reviewer: Jonathan Loveday / Codes: / Published: 09/07/2019 / Reviewed: 02/12/2025
ECGs can be challenging, right? And so can children. Add the two together and..arrghh Paediatric ECGs!!
No need for the heartache though, take things one step at a time and see how things unfold.
Indications
Why on earth would you want to do an ECG in a child, anyway? Well, here’s a list of things that come to mind:
- Collapse or seizure: could it have been a dysrhythmia?
- Family history of sudden cardiac or unexplained death: long QT? Brugada?
- Clinical presentation suggesting cardiac failure: weight loss or failure to thrive, SOB, sweating (particularly on feeding)?
- Unexplained tachycardia or suggestion of arrhythmia: palpitations, poor perfusion, SOB?
- Chest pain on exertion
- Drug ingestion or poisoning
How to perform an ECG (easier said than done)
For older children, the “how” is just like you would with an adult. Younger children are more of a challenge though. It’s worth putting the limb leads on the trunk instead (at the root of each limb) to help eliminate artefactual changes that come with movement. You may also need to employ some distraction techniques (here‘s a blog from St Emlyn’s for some inspiration). The paediatric heart is right-side dominant, so you’ll also need to record an additional V4R lead.

ECG placement courtesy of LITFL
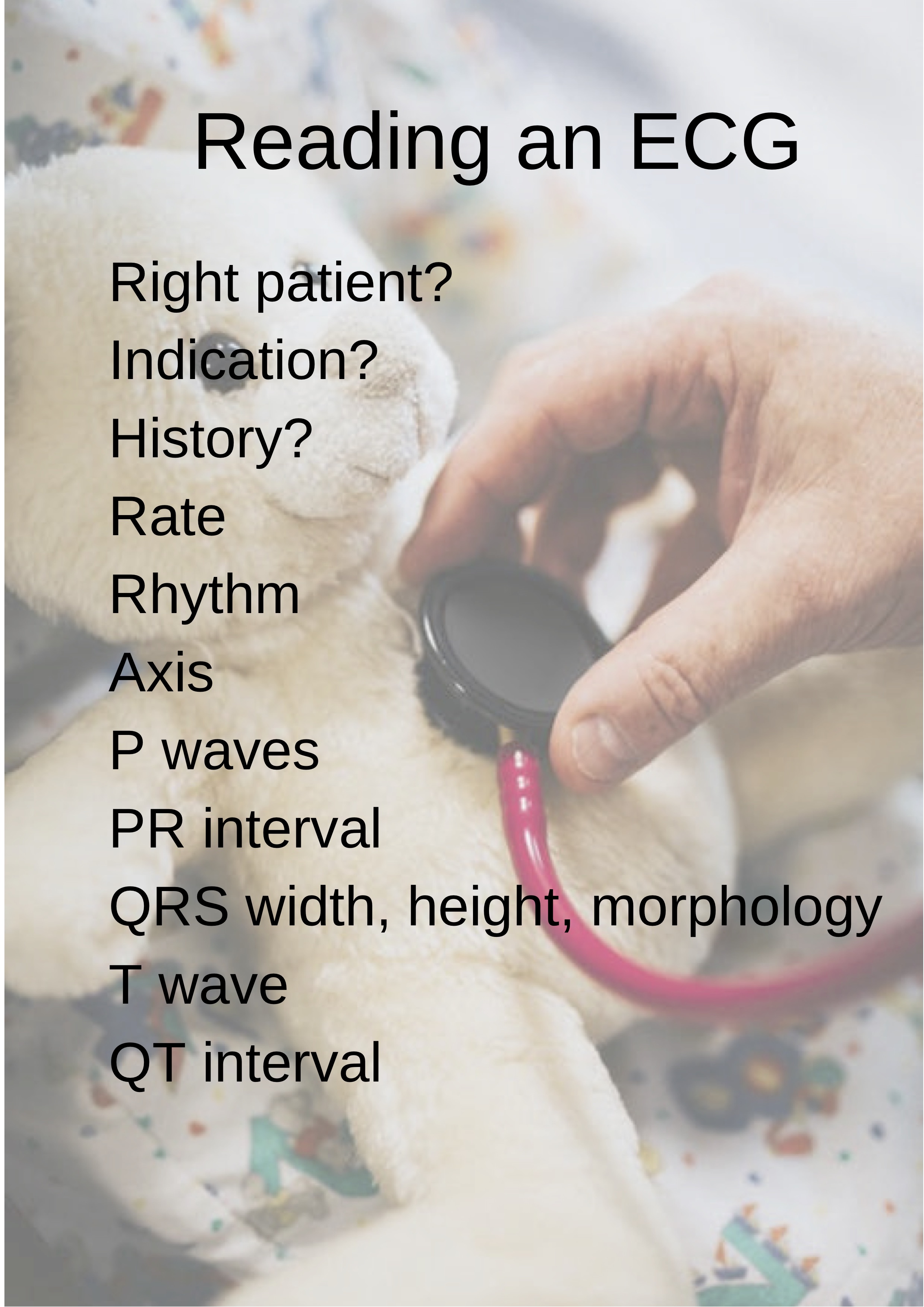
Have a system
You already knew that, didn’t you? Like with most things, a system helps to make sure you don’t miss things, particularly when there’s an abnormality jumping out at you.
Small hearts
The foetal circulation is very different to the adult circulation. Instead of a dominant left ventricle pumping oxygenated blood from the pulmonary circulation to the systemic circulation, the right side of the heart is dominant. Blood is oxygenated instead in the placenta and delivered to the right side of the heart via the umbilical vein, the ductus venosus and then the IVC. Some is shunted across from the right atrium to the left atrium through the foramen ovale. More is shunted from the pulmonary artery to the aorta via the ductus arteriosus, so a good proportion of the oxygenated blood received by the right atrium ends up in the systemic circulation, bypassing the fluid-filled foetal lungs. The remainder, ending up in the pulmonary circulation, is under pressure as the vascular resistance in the lungs is high. So, the right ventricle is bigger and thicker than the left, and the foetal heart has a right-sided axis.
After birth, when the lungs fill with air, the pulmonary vascular resistance falls and the foramen ovale and ductus arteriosus close. Gradually, as the child grows, the left ventricle grows and takes over, so the axis moves to the left.

In young children there’s a dominant R wave in V1-3, sometimes with an rSR1 pattern in V1. Q waves are present in the inferior and left precordial leads. T wave inversion is present in leads V1-3. Sinus arrhythmia is common. The heart rate is also faster, of course, with narrower complexes and shorter intervals.

Normal Paediatric ECG from LITFL
In early childhood, as the axis moves to the left, the R waves in leads V1-3 become more “adult”, although the T wave inversion and sinus arrhythmia persist.
In adolescence, the ECG looks much more like the adult ECG, although sinus arrhythmia is still common, as is benign early repolarisation.

LITFL have an excellent ECG library and here is an example from their site
Some Common Abnormalities
Sinus tachycardia
Sinus tachycardia is the commonest paediatric dysrhythmia. Fever, pain, anxiety, fear and running around the waiting room are all reasons we see every day for children to get a sinus tachycardia. Of course, it can also be a sign of compensation and an attempt to increase cardiac output is the tachycardia appropriate? What other signs and symptoms might give us a clue? Does the tachycardia resolve when we manage the fever, pain or fear?
SVT
SVT is usually a little faster: more than 220 bpm in an infant and more than 180 bpm in a child. It has a more abrupt onset (and end) than sinus tachycardia, with less beat-to-beat variation and little or no response to stimulation such as pain or movement. Paroxysmal SVT is fairly common, especially in infancy, where it is often due to an accessory pathway, such as in WPW syndrome. Beware of the infant with a “high” tachycardia and poor feeding who may have an underlying SVT and won’t present in the typical way.

Sinus bradycardia
Sinus bradycardia is common in sleep (and athletic adolescents).
Congenital malformations
Congenital malformations can cause many different ECG changes, including conduction abnormalities, signs of LVH or RVH and rhythm disturbances.
Myocarditis and cardiomyopathy
Myocarditis and cardiomyopathy can give changes associated with RVH or LVH, ST segment changes and abnormal QRS morphology.
Long QT
Long QT (normal= 460): QTc needs to be measured manually on lead II or V5 with Bazetts formula as the heart rate tends to lie outside the 60-100bpm interval and so the actual QT measurement is unreliable. Also make sure it is estimated on 3 different QT measurements due to the beat-to-beat variation which is common in children.
Right bundle branch block (partial or complete), supraventricular ectopics and Wenckebach
Right bundle branch block (partial or complete), supraventricular ectopics and Wenckebach can all be benign as with most things, your history and clinical evaluation are key!
Further reading
- RCEMLearning blog: Doctor can you cast your eyes over this ECG for me?.
- RCEMLearning Reference: Brugada Syndrome
- DFTB: Congenital Heart Disease in the ED
- DFTB: ECG intervals by age.
- DFTB: Normal ECGs various ages.
- LITFL: Paediatric ECG