
Author: Jason L Louis / Editor: Jason M Kendall / Reviewer: Martin Dore, Josh Davison, Emma Everitt / Codes: A5 / Published: 22/01/2024
Context
Although they can occur at any age, cervical artery dissections are the cause of around 13% of ischaemic strokes in patients under 45 years of age and the condition is likely to be underdiagnosed.1 This condition is easily missed and the key to making the diagnosis is having a high index of suspicion based on the clinical presentation.
Cervical artery dissection encompasses dissections of both the carotid and vertebral arteries. These conditions have similar aetiology but different clinical presentations. The combined incidence is around 3.5-4.5 per 100,000 with carotid artery dissection being twice as common as vertebral artery dissection2.
Pathophysiology
The basic lesion in cervical artery dissection is an intramural haematoma in the vessel wall. This may arise from haemorrhage from the vasa vasorum, or can be the result of a tear in the intima of the vessel giving rise to an intimal flap. The intramural haematoma can narrow the vessel lumen or cause an aneurysmal dilatation. Clinical features occur through 2 mechanisms:
- Both low flow through a stenosed vessel and intimal damage can cause thrombus formation and this leads to embolic neurological sequelae.
- The haematoma, with or without aneurysm formation, can cause symptoms from compression of adjacent structures.
Risk factors
The development of a cervical artery dissection is usually associated with either trauma or connective tissue disease and most commonly occurs between 35-45 years of age. The trauma involved can be trivial and there have been reports of cases following sneezing and yoga.
Risk factors include3:
- Trauma
- Respiratory tract infection
- Fibromuscular dysplasia
- Cystic medial necrosis
- Marfan syndrome
- Ehlers-Danlos syndrome
Clinical presentation
The initial symptom is usually pain with headache occurring in around 70% of patients.3 In vertebral artery dissection this is often occipital pain extending into the neck and in carotid dissection can be headache, neck or facial pain. The pain is on the same side as the dissection.
Focal neurological signs then follow in about 60% of patients.3 These often develop several days after the onset of pain and display different patterns depending on the vessel involved.
(i) Vertebral Artery Dissection:
This affects the posterior circulation and most often presents as a lateral medullary syndrome due to emboli in the posterior inferior cerebellar artery (see figure).
This causes:
- ipsilateral facial pain and temperature sensory loss (spinal trigeminal nucleus)
- contralateral pain and temperature sensory loss from the body (lateral spinothalamic tract after decussation)
- dysphagia and dysarthria (nucleus ambiguus motor fibres of CN IX and X)
- ataxia (cerebellar peduncle)
- vertigo (vestibular nuclei)
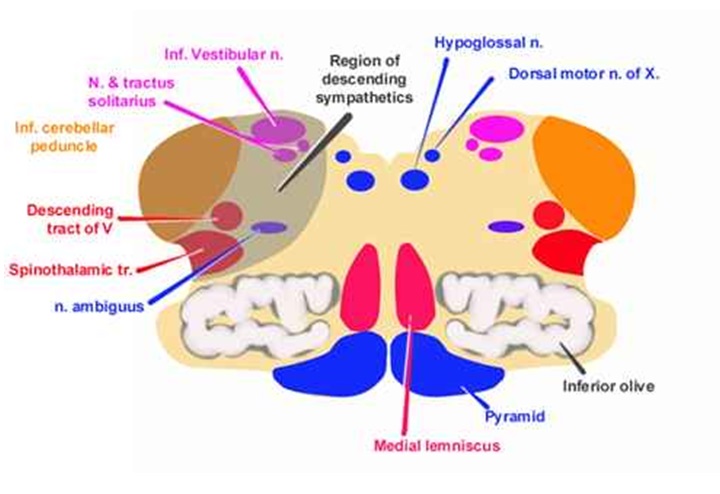
Patients may also have a Horners syndrome cause by ischaemia of the descending sympathetic fibres.
(ii) Carotid Artery Dissection:
This may result in focal weakness and/or sensory loss and amaurosis fugax. There may be a carotid bruit. Carotid artery dissections can also cause a Horners syndrome due to compression of the sympathetic fibres travelling with the internal carotid. In this case sweating is preserved as this is regulated by sympathetic fibres in the external carotid plexus.

This MRA image shows intramural haematoma and narrowing of the lumen of the left vertebral artery (arrow).
Differential diagnoses will vary according to the presence or absence of pain and trauma but include:
- Migraine
- Stroke
- TIA
- Subarachnoid haemorrhage
- Traumatic brain injury
Investigative options include:
Non-contrast CT scan
Because many patients will present with headache and neurological symptoms after a head or neck injury, the initial investigation performed is often a non-contrast CT scan.
This will usually be normal, and this can be falsely reassuring, unless the clinician has a high degree of suspicion for a cervical artery injury.
CT angiography (CTA) may provide a higher yield for those in whom the clinical suspicion of dissection is high. It may also be useful in trauma patients who are undergoing CT for other indications. In the UK MR angiography is the investigation of choice and with advances in scanner technology the sensitivity of MRA is approaching that of the gold standard of cerebral angiography.4
Doppler ultrasound is fast, convenient and non-invasive and will demonstrate abnormal flow in around 90% of patients with either vertebral or carotid artery dissection (although it is technically difficult to scan the distal internal carotid).5 This is therefore a rule in investigation and positive results should be followed up with definitive imaging as below.
Why we use imaging
In the UK, MRA is the investigation of choice and with advances in scanner technology the sensitivity of MRA is approaching that of the gold standard: cerebral angiography.
Both CTA and MRA will usually reveal a decrease in the diameter of the affected vessel and, possibly, signs of an intramural haematoma.
It is less common to see an intimal flap.
Although still the gold standard investigation, cerebral angiography is invasive and not routinely performed in the UK.
It is probably best reserved for patients in whom there is a high clinical suspicion, but a normal MRA.
Once cervical artery dissection has been confirmed the mainstay of treatment is anticoagulation. The have been no randomised controlled trials examining anticoagulation and its use is only supported by case reports, however as the neurological sequelae are caused by thromboembolism it seems a sensible approach. In patients with head trauma it is important to exclude haemorrhage with a CT brain scan prior to instituting anticoagulation.
As there are inherent risks associated with anticoagulation, in some patients, it may be decided that treatment with aspirin alone is the best approach, particularly those without neurological signs.
Endovascular stenting is a further option, particularly for patients with a contraindication to anticoagulation.
Mortality is around 5-10%, but of those surviving 75-80% will make a complete recovery.6
The main pitfall in managing this condition is not suspecting it in the first place. If not initially suspected on purely clinical grounds cervical artery dissection should be considered in any patient with a head injury and neurological symptoms and/or signs who has had a normal CT brain scan.
Cervical artery dissection can present as an acute stroke, with focal neurological signs but no other associated features, often in a young patient. Some such patients will meet the criteria for thrombolysis.
The clinical trials of thrombolysis in acute stroke did not attempt to differentiate these patients from those with other causes of stroke. If the clinical picture is therefore of stroke in a young patient but there are no other clinical features to suggest a dissection, it is reasonable to proceed with thrombolysis.
- Chan MTY, Nadareishvili ZG, Norris JW. Diagnostic strategies in patients with ischaemic stroke in Canada. Can J Neurol Sci. 2000;27:120-124.
- Beletsky V, Nadareishvili Z, Lynch J et al. Cervical artery dissection: time for a clinical trial?. Stroke. 2003;34:2856-2860.
- Schievink W, Mokri B, OFallon M. Recurrent spontaneous cervical artery dissection. N Enlg J Med. 1994;330:393-397.
- Kennedy F, Lanfranconi S, Hicks C, et al. Antiplatelets vs anticoagulation for dissection: CADISS nonrandomized arm and meta-analysis. Neurology 2012; 79:686.
- Chowdhury MM, Sabbagh CN, Jackson D, et al. Antithrombotic treatment for acute extracranial carotid artery dissections: a meta-analysis. Eur J Vasc Endovasc Surg 2015; 50:148.
- Sturzenegger M, Mattle HP, Rivoir A et al. Ultrasound findings in carotid artery dissection: analysis of 43 patients. Neurology. 1995;45:691-698.
- Biousse V, DAnglejan-Chatillon J, Touboul PJ et al. Time course of symptoms in extracranial carotid artery dissections: a series of 80 patients. Stroke. 1995;26:235-239.