
Authors: Shella Kwok, Riad Hosein / Editor: Lauren Fraser / Codes: / Published: 28/11/2022
Pelvic fractures are one of the potentially life-threatening injuries identified during primary survey of patients with major trauma. A pelvic fracture can result in significant blood loss that is difficult to control and can lead to death if not managed appropriately. Early suspicion, identification and management of pelvic fractures in the Emergency Department are essential for reducing blood loss and to decrease mortality.
In studies of patients with blunt trauma, the prevalence of pelvic fracture ranges from 5% to 11.9%. Mortality rate has been reported to be between 7.6% and 19%. An open pelvic fracture carries a much higher mortality rate and approaches 50%1. There is a bimodal age distribution of pelvic injury:- incidence at 15-30 years old mainly caused by road traffic accident and over 60 years old caused by falls.
Learning Bite
Pelvic fracture is a marker of considerable energy transfer. Assess for associated visceral injuries and manage blood loss. An open pelvic fracture carries a much higher mortality rate approaching 50%.
Introduction

Fig. 1 Pelvis and Hip Anatomy Hank Grebe/Shutterstock.com
The pelvis is a ring structure made up of 3 bones:
- 2 X innominate bones (Each innominate bone is formed by fusion of the 3 ossification centres named ILIUM, ISCHIUM and PUBIS at the Triradiate cartilage, which closes at around 15-17 years old to form a cup-shaped socket known as the acetabulum.)
- 1 X sacrum. Joined anteriorly at the symphysis and posteriorly at the paired sacroiliac joints.
Learning bite
The acetabulum is made up of all 3 parts of ilium, ischium and pubis. It is important to consider an acetabulum fracture as a potential complex pelvic fracture.
Stability of pelvis
The following 4 ligaments are important for providing stability of the pelvis:
- Sacroiliac ligaments (strongest ligament in the pelvis and provides most of the stability)
- Sacrotuberous ligaments (resists vertical shearing forces
- Sacrospinous ligaments (resists external rotational forces)
- Pubic symphysis ligament

Fig. 2 Posterior view of pelvic ligaments. OpenStax College via Wikimedia Commons
Structures of the pelvis
The human pelvis represents a complex anatomical region shared by organs of the gastrointestinal tract, genitourinary tracts and the reproductive system. An intricate neurovascular network accompanies all these structures that often requires collaboration of interdisciplinary teamwork in the presence of injury.
Blood vessels
1.Arteries: main arteries are highlighted in red.

The abdominal aorta descends towards the pelvis and divides at L4 (surface marking of the umbilicus) into left and right common iliac arteries which branch further into the external and internal iliac arteries. The external iliac arteries continue to supply the lower extremities as femoral arteries and other branches. The internal iliac arteries branch and remain within the pelvic region to supply blood to pelvic organs, gluteal muscles and the perineum.
2. Veins

The anatomical position of the pelvic veins follows the same path of the arteries and mostly take their names. The femoral vein reaches the pelvis through the inguinal ligament and becomes the external iliac vein. Important to note is the presence of pre-sacral venous plexus, which is vulnerable to profuse bleeding in pelvic injury.

Learning bite
Pre-sacral venous plexus bleeding can be profuse and difficult to control in major pelvic injury.
Nerves
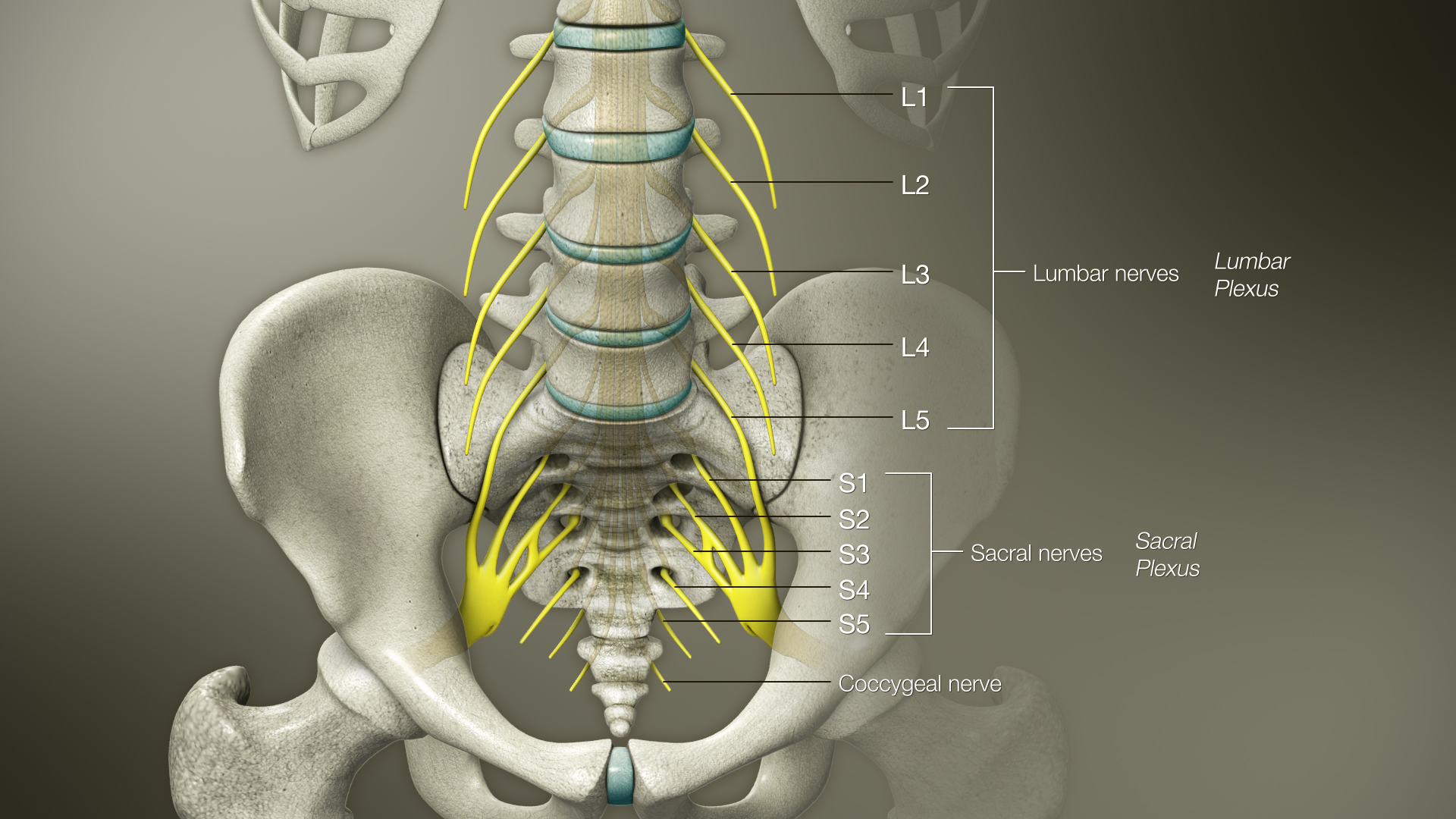

The nerves exiting L4 and L5 form the lumbo-sacral trunk and merge with the sacral plexus, which consists of the sacral nerves from S1 to S4. The sacral plexus descends along the posterior pelvis. The main nerves of the sacral plexus include:
- Sciatic nerve which is the largest human nerve formed by branches of L4-S3. The nerve innervates the muscles of the posterior thigh and the hamstring portion of the adductor magnus. It also innvervates the muscles of the leg and foot via its terminal branches.
- Pudental nerve which innervates the muscles and skin of perineum
- Superior and inferior gluteal nerves innervate the gluteal muscles
Learning bite
The sciatic nerve arises from the sacral plexus, which can be affected by a pelvic injury.
Lymphatic system

The pelvis has an extensive lymphatic system made of large number of lymph nodes and lymphatic ducts. Lymph nodes are mostly located along blood vessels. Their function is to combat potential infections.
Organs


Fig. 9 &10 Sagittal views of Male and Female Pelvic Organs. BruceBlaus via Wikimedia Commons
Pelvic fractures can be suspected by the identification of ecchymosis over the iliac wings, pubis, labia, or scrotum. Pain on palpation of the pelvic ring is an important finding in alert patients, important to note it is NOT recommended to spring the pelvis. In addition, assessment of peripheral pulses can identify vascular injuries. Inspect the flank, scrotum, urethral meatus, and perianal area for blood, swelling, and bruising. Laceration of the perineum, vagina, rectum, or buttocks may be associated with an open pelvic fracture in blunt trauma patients. Skin folds in obese patients can mask penetrating injuries and increase the difficulty of assessing the abdomen and pelvis.
Learning bite
Pelvic organ injury can be difficult to diagnose and requires complex multi-disciplinary management.
Interpretation of pelvic x-ray

You should start by tracing three rings on the AP pelvic x-ray: the main pelvic ring and two obturator foramen rings.
If any of the rings are disrupted, think fracture and look for a second one.

If either joint space is widened, think main pelvic ring fracture.
Learning bite
Trace 3 rings and measure 3 joint spaces on a pelvic X-ray to assess for ring fractures.
Here are two useful resources for further details on interpretation of pelvic x-ray:
- How to Read Hip and Pelvis X-Rays. Taming the RSU. Emergency Medicine tamed. 2014.
- Jones J, Yap J. Pelvic radiograph (an approach). Radiopaedia. 2014. Last revised 2022.
Mechanism of pelvic injury can be broadly divided into two types: Low-energy and High-energy.
1. Low-energy injury resulting in isolated fracture with an intact pelvic ring. Common examples are:
- Avulsion fracture (Usually in young athletes with sudden muscular contraction. Common sites are ASIS/AIIS/Pubis)
- Direct fracture (Usually from a low impact fall. Common sites are the iliac crest or ischium)
- Stress fracture (Caused by osteoporosis or malignancy. Common sites are the pubic rami or the sacro-iliac joint)

These types of low-energy injury are considered stable and can usually be managed with analgesia and rest.
Learning bite
It is important to be cautious when assessing low-energy injuries in the elderly, especially in females >80 years old where low energy impact is a main cause of pelvic ring injury.
2. High-energy injury resulting in disrupted pelvic ring

As mentioned before, the pelvis can be considered as a ring structure, which means a break in one area of the ring is usually accompanied by a break in another area of the ring. This depends on the mechanism and direction of force:
A. Anteroposterior Compression (APC) (Grade 1-3)
Usually results from frontal or head-on collision road traffic accidents. Force is transmitted from the anterior pelvis through to the posterior. This type of injury causes a widening of the pelvic ring as the pubic symphysis separates. Widening of the sacroiliac joints at the back of the pelvis can also occur, causing internal bleeding. This type of fracture is also known as open book fracture.

B. Lateral Compression (LC) (Grade 1-3)
Side on impact causing lateral compression of the pelvic ring to buckle and break. This is the most common type of pelvic fracture from a motor vehicle collision.

There is a theoretical risk that a pelvic binder may worsen this type of fracture, however it is impossible to identify types of injury by clinical assessment alone. It is better to apply a pelvic binder to stabilise the fracture and control potential bleeding.
C. Vertical Shear (VS)
Fall from a height on one leg or axial load mechanism causing displaced fractures of the anterior rami and posterior column with SI joint dislocation. This type of injury is vertically unstable and always requires operative management. Traction may be required to stabilise the hemipelvis.

D. Complex Pattern Injury
When pelvic injuries involve a combination of two or more of the fractures described above, these are classified as complex pattern injuries and are completely unstable.

Classification of pelvic injury
There are various system of classification, the two most commonly used are:
1.Young-Burgess Classification more common and useful in ED as it is based on mechanism and stability.

2. Tile Classification based on pelvic stability and useful for guiding pelvic reconstruction.

Learning Bite
Young-Burgess Classification Type II and III/ Tile B and C are all unstable pelvic fractures requiring surgical intervention
Introduction
- Immediate management
- Control of haemorrhage
- Use of pelvic binder
- REBOA
- Management of stable VS unstable fracture
- Management of closed VS open fracture
- Other injuries
Immediate management
- Coordinated and structured approach (eg. ATLS approach)
- C-ABCDE assessment as per any other patients
- Pelvic stabilisation as part of C (eg. Pelvic binder)
- Examine perineum, genitalia and rectum for blood which suggests an open pelvic fracture
- DO NOT spring/rock the pelvis may dislodge clots and promote further bleeding
DO NOT log roll if there is suspicion of pelvic fracture as it can cause dislodge clot and cause further haemodynamic compromise (unless there are active bleeding stab wounds suspected on the back or airway compromise. If necessary to log-roll, maximum 15 tilt should be adopted). Below is guidance taken from NICE Guideline 37 (3).
- If bleeding is suspected, give IV tranexemic acid 1g bolus followed by infusion if within 3 hours of injury and activate your local Major Haemorrhage Protocol for an unstable patient requiring blood transfusion
- Analgesia: IV morphine first line/ IN diamorphine or ketamine (4)
- Cross match blood along with organising other laboratory blood tests (VBG, lactate, FBC, U&E, Clotting profile)
- Imaging with CT. Contrast extravasation on CT is also called CT blush which suggests active bleeding during the arterial phase and is likely to need angiographic embolization.

Learning bite
Avoid unnecessary movement of the patient. DO NOT spring the pelvis on examination and DO NOT log-roll if pelvic injury suspected.
1a Control of haemorrhage
- Haemostatic resuscitation
- Pelvic binder
- Intervention radiology for angiography embolization if arterial bleed present
- Packing in theatre primarily stems venous bleeding or is used for unstable patients (pre-peritoneal packing or retroperitoneal packing) or if embolization has been unsuccessful
- Damage control surgery usually occurs first before trying to fix
- Mechanical stabilisation of pelvic fracture by external fixation
Leading cause of death in pelvic injury is BLEEDING!
Venous haemorrhage is thought to account for nearly 90% of pelvic fractures and arterial haemorrhage only 10%5. True pelvic volume is about 1.5L but this volume increases with disruption of the pelvic ring. Haemorrhage from a pelvic fracture is essentially bleeding into a free space, which is capable of accommodating the patients entire blood volume without exerting a tamponade effect. Blood can escape into the peritoneum, thighs and retro-peritoneal space which can accumulate 5L in volume with only a pressure rise of 30mmHg5.
Learning bite
Nearly 90% of pelvic fracture bleeding is venous in origin.

1b Use of pelvic binder
A range of pelvic binders are available which aim to reduce and stabilise pelvic fractures. Currently there is insufficient evidence to support one device over the other. If no device is available, use a bed sheet to wrap around the pelvis. Pelvic binders also help with:
- Prevention of re-injury from pelvic motion
- Decreasing pelvic volume
- Decreasing pain
- Controling bleeding
Application of pelvic binder: SPLINT TO SKIN!

- Straighten both legs
- Apply to skin directly
- At the level of greater trochanter
- Sams Sling is commonly found in most EDs 3 sizes available (small, standard and large. If in doubt, use the standard size which is designed to fit 95% of the population)
- Pelvic binders are compatible with CT and MRI
- If appropriately applied the feet should be internally rotated
- Video for application of pelvic binder
Learning bite
It is important to identify the correct landmark of the greater trochanters to apply the pelvic binder, otherwise it is ineffective. Only 50% were positioned correctly according to a survey done in 20186.
When to put the pelvic binder on?
See guidance below from NICE Pathway and Royal College of Surgeons of Edinburgh on when to apply the pelvic binder3.


Essentially apply the pelvic binder if in doubt or if pelvic fracture is suspected.
Removal of pelvic binder
The pelvic binder can be removed as soon as possible if4:
- there is no pelvic fracture, or
- a pelvic fracture is identified as mechanically stable, or
- the binder is not controlling the mechanical stability of the fracture, or
- there is not further bleeding and coagulation is normal
The pelvic binder should be removed within 24 hours to prevent pressure ulcers from developing.
It is important to closely monitor the patients haemodynamic status and repeat the pelvic x-ray post binder removal because a well-applied pelvic binder can mask fracture. See example below of pelvic x-ray with and without binder.

Sometimes even the CT will appear normal with the pelvic binder on.


Learning bite
Monitor the patients status closely and repeat the pelvic x-ray post pelvic binder removal.
REBOA
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) is increasingly used as a non-invasive clamp of the aorta. Balloon inflation in zone 3 (from the lower renal artery to the aortic bifurcation) can be performed to stop on-going bleeding after severe pelvic trauma with life-threatening haemorrhage. Studies support the use of REBOA as a bridge to definitive haemostatic treatment after severe pelvic trauma7.
Learning bite
REBOA can be considered in severe pelvic trauma and life-threatening haemorrhage.
Management of stable VS unstable pelvic fracture
Definition of stable injury: able to withstand physiological forces without significant displacement (ie. <1cm). Usually managed conservatively.
Unstable pelvic fractures can be unstable vertically or rotationally. Operative management is required with either External Fixation or Open Reduction with Internal Fixation (ORIF).
Learning bite
All unstable pelvic fractures require operative management.
Management of close VS open pelvic fracture
- Give antibiotics as soon as possible if an open pelvic fracture is suspected
- Consider tetanus vaccine or immunoglobulin if a wound is prone to contamination
- An open pelvic fracture carries a much higher mortality rate and complication rate
- Examination for blood in vagina/urethral meatus/rectum are of utmost importance to rule out presence of an open pelvic fracture
Useful short guide on The Management of patients with Pelvic Fractures by the British Orthopaedic Association Audit Standards for Trauma (BOAST) here.
Learning bite
Presence of any vagina/urethral/rectal injury with a pelvic fracture signifies an open pelvic fracture.
Other injuries
Genitourinary injuries (5-10%)
- Urethral injury (anterior: penile/bulbar usually caused by straddle injury, posterior: membranous/prostatic usually caused by crushing force to the pelvis in RTC)
- Bladder rupture (intraperitoneal/ extraperitoneal)
The presence of blood at the urethral meatus, ecchymosis or hematoma of the scrotum and perineum are strongly suggestive of urethral injury, although these signs may be absent immediately after injury. Palpation of the prostate gland is not a reliable sign of urethral injury. Gross haematuria or blood stained urine is also an indication of trauma to the genitourinary tract (including the kidney, ureters, and bladder). The absence of haematuria does not exclude an injury to the genitourinary tract. Presence of any of the above findings MANDATES a catheter retrograde cystogram/ urethrogram to investigate for GU injuries. This can be done via urethral/suprapubic catheter. Consult urology specialist for advice prior to inserting catheter if urethral injury is suspected. Do not place a urinary catheter in a patient with a perineal hematoma or blood at the urethral meatus before a definitive assessment for urethral injury.
Useful guide from BOAST on The Management of Urological Trauma Associated with Pelvic Fractures here.
Gastrointestinal injuries (5%)
- May need urgent bowel diversion or a de-functioning stoma and washout
- Urgent senior general surgical input is required
- Any colostomy should be sited in an upper abdominal quadrant remote from potential definitive pelvic surgical fixation approaches
- Risk of death from secondary sepsis and bowel content contamination
In patients who have sustained blunt trauma, the goals of the rectal examination are to assess sphincter tone and rectal mucosal integrity and to identify any palpable fractures of the pelvis. In patients with penetrating wounds, the rectal examination is used to assess sphincter tone and to look for gross blood, which may indicate a bowel perforation.
The gluteal region extends from the iliac crests to the gluteal folds. Penetrating injuries to this area are associated with up to a 50% incidence of significant intra-abdominal injuries, including rectal injuries below the peritoneal reflection. These wounds mandate an evaluation for such injuries.
Vaginal injuries (<5%)
Bony fragments from pelvic fracture or penetrating wounds can lacerate the vagina. Perform a vaginal exam when injury is suspected, such as in the presence of complex perineal laceration, pelvic fracture, or transpelvic gunshot wound. In unresponsive menstruating women, examine the vagina for the presence of tampons left in place, they can cause delayed sepsis.
Learning bite
Pelvic fracture can be associated with complex injuries requiring multispecialty input.
Patients should be followed-up in specialist pelvic units to ensure full advice is available for different aspects of care including pain management, physical, urological and sexual disabilities.
Complications of pelvic injury include:
- Morel-Lavalle Lesion (Morel Lavalle Lesions (MLL) are uncommon shearing injuries resulting in separation of the skin and subcutaneous tissue from the underlying fascia. Essentially it is a closed internal degloving injury- consult plastic surgery).


Fig.28 Image via Radiopaedia.org. Case courtesy of Dr Matt Skalski
- Thromboembolism
- Pelvic infection
- Osteomyelitis
- Sciatic nerve injury
- Urological stricture/incontinence/impotence
- Persistent pain from malunion
Learning bite
Pelvic injury can lead to multiple complications and should be followed up in specialist pelvic units.
-
- Its important to know the mechanism of injury.
- Clinical examination for pelvic injury is unreliable if patient GCS <15 or if there is a distracting injury.
- On the contrary, if the patient is alert and awake, painless straight leg raise can be incorporated into initial examination to exclude pelvic fracture.
- Springing of pelvis and log-rolling should not be done as blood clot can be dislodged causing haemodynamic instability.
- The pelvic binder is frequently applied incorrectly and too high. It should be applied directly to the skin and at the level of the greater trochanter, which is lower than the trousers waistline and should be at a similar level to testicles for males. Too often the pelvic binder is applied on top of the clothes, which can cause pressure necrosis and impedes physical examination of the perineum area.
- Forgetting to request a post binder removal pelvic x-ray. Pelvic binder can mask a pelvic fracture on CT or X-ray.
-
-
- Lee C, Porter K. The prehospital management of pelvic fractures. Emerg Med J. 2007 Feb;24(2):130-3.
- Molire S, Dosch JC, Bierry G. Pelvic, acetabular and hip fractures: What the surgeon should expect from the radiologist. Diagn Interv Imaging. 2016 Jul-Aug;97(7-8):709-23.
- National Institute for Health and Care Excellence. Fractures (complex): assessment and management. NICE [NG37]. 2016. Last updated Nov 2017.
- Nickson C. Pelvic Trauma. Life in the Fast Lane, 2020.
- White CE, Hsu JR, Holcomb JB. Haemodynamically unstable pelvic fractures. Injury. 2009 Oct;40(10):1023-30.
- Naseem H, Nesbitt PD, et al. An assessment of pelvic binder placement at a UK major trauma centre. Ann R Coll Surg Engl. 2018 Feb;100(2):101-105.
- Pieper A, Thony F, Brun J, Rodire M, et al. Resuscitative endovascular balloon occlusion of the aorta for pelvic blunt trauma and life-threatening hemorrhage: A 20-year experience in a Level I trauma center. J Trauma Acute Care Surg. 2018 Mar;84(3):449-453.
- Scott I, et al. The Pre-Hospital Management of Pelvic Fractures: Initial Consensus Statement. The Royal College of Surgeons of Edinburgh.
- Teach me anatomy. The Pelvis.
- Lierse, W. Structural and Functional Anatomy of the Pelvis. In: Applied Anatomy of the Pelvis. Springer, 1987. Berlin, Heidelberg.
- Khurana B, Sheehan SE, Sodickson AD, Weaver MJ. Pelvic ring fractures: what the orthopedic surgeon wants to know. Radiographics. 2014 Sep-Oct;34(5):1317-33.
- Tile M. Acute Pelvic Fractures: I. Causation and Classification. J Am Acad Orthop Surg. 1996 May;4(3):143-151. doi: 10.5435/00124635-199605000-00004.
- Landing page image from: Wiznia DH, Wang M, et al. Traumatic Testicular Dislocation Associated with Lateral Compression Pelvic Ring Injury and T-Shaped Acetabulum Fracture. Case Rep Orthop. 2016;2016:9706392.
-
Additional Resources